Published Jan 03, 2024 | 11:00 AM ⚊ Updated Jan 04, 2024 | 5:28 PM


Rural women in India. Representational image. (Wikimedia Commons)

The World Health Organization (WHO) defines health as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity. It is well known that several social determinants contribute directly or indirectly to health outcomes.
Southern states are generally considered to be more prosperous with better health and education outcomes and a higher standard of living. Most states in the South have slowed down population growth.
Except for Telangana, the four southern states contribute much of the country’s economic activity. Kerala and Tamil Nadu are among the wealthiest states in the country, with a mean age of 30 years, a fertility rate lower than the mean replacement rate, and a life expectancy similar to middle-income countries.
Andhra Pradesh and Telangana are the fastest-growing economies with abundant natural resources. Despite a lower per capita income, Kerala scores high on the Human Development Index. Tamil Nadu and Karnataka have shown marked improvement.
This article highlights some indicators that influence health outcomes and the need for states to plan interventions holistically. For instance, a woman’s access to education, contraception, or better living conditions within her home can affect the health and nutritional status of herself and her children.
Picking one health issue, for example, anaemia, and planning one single intervention, for example, fortification, may not lead to the desired outcome in the long run as much as a holistic approach.
This article highlights some indicators from the National Family Health Survey-5 (NFHS) and the Comprehensive National Nutrition Survey (CNNS 2019) for Telangana, Andhra Pradesh, Karnataka, Kerala, and Tamil Nadu. Indicators for two North Indian states — Bihar and Gujarat — are also included.
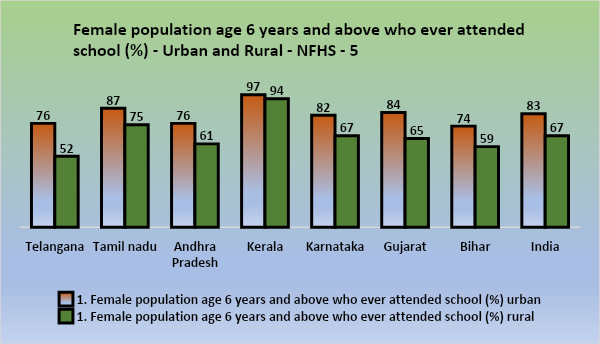
Female population age 6 years and above who ever attended school (%) – Urban and Rural – NFHS 5. (Supplied)
Women’s education can affect their access to jobs, income, housing, nutrition, education for their children, and healthcare.
There is a need to raise the bar on educational inputs in rural areas across all the states assessed. In Kerala, more than 90 percent of women aged 6 years and above have attended school.
The population-level sex ratio depends on three factors: The sex ratio at birth, the differential mortality rates between sexes at different ages, and losses/gains through migration.
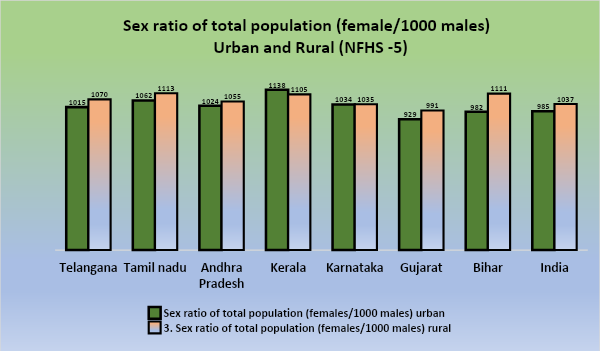
Sex ratio of total population (female/1000 males) – Urban and Rural – NFHS 5.
Experts believe that the Census, which showed a ratio of 933 women per 1,000 men in 2011, is a more reliable estimate of the population sex ratio than the NFHS, which may not be a representative sample and is influenced by migration behaviours.
The sex ratio at birth tends to be male-biased at 1,050 males per 1,000 females but becoming more female preponderant in older age groups. Although females who receive good nutrition and healthcare are documented to have lower mortality than males, this can become inverse because of discriminatory practices and negligence.
A lower sex ratio at birth is often attributed to prenatal sex determination, and selective abortion is more likely to increase with birth order. With the development of the country or state, this ratio can improve.
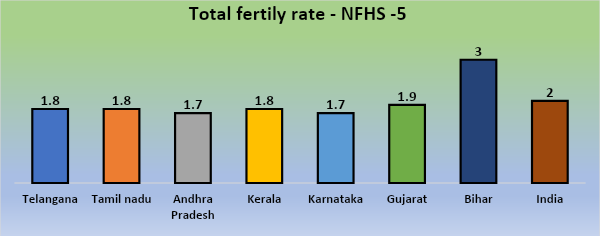
Total fertility rate – NFHS 5. (Supplied)
Total Fertility Rate (TFR) indicates the average number of children expected to be born to a woman during her reproductive span of 15-49 years. High fertility is associated with an increased risk of maternal morbidity and mortality, fewer opportunities to work outside the home or improve the family’s economic and social status.
The replacement level for TFR is usually 2.1 children per woman. Further drop over time can lead to an ageing population, which requires other specific health and other interventions. Bihar has a high TFR of 3, which points towards the need for investing more in improving women’s access to education, literacy, and healthcare, including contraception. Most southern states show a TFR of around 1.8, which is less than the replacement level.
Infant Mortality Rate (IMR) is defined as the number of deaths of children under the age of 1 year per 1,000 live births for a given year. India’s IMR is 34 per 1,000 live births, with wide variation among states.
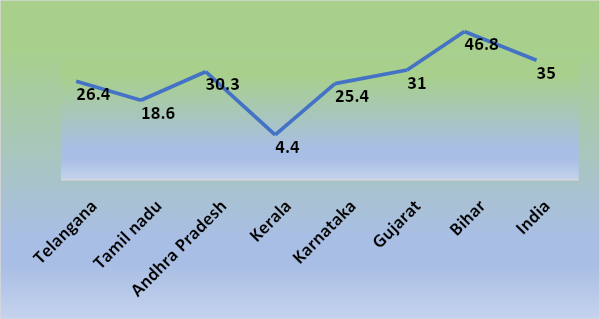
Infant mortality rate – NFHS 5. (Supplied)
Kerala’s IMR of 4.4 is comparable to that of high-income countries. Bihar has a high IMR of 46.8. Leading causes of IMR include preterm birth, low birth weight, neonatal infections, birth asphyxia, birth trauma, pregnancy-related complications, etc. Between age 1 – 59 months, pneumonia and diarrhoeal diseases are the biggest contributors. These are further linked to a host of factors, such as inadequate healthcare facilities, poor education, literacy, nutrition, etc.
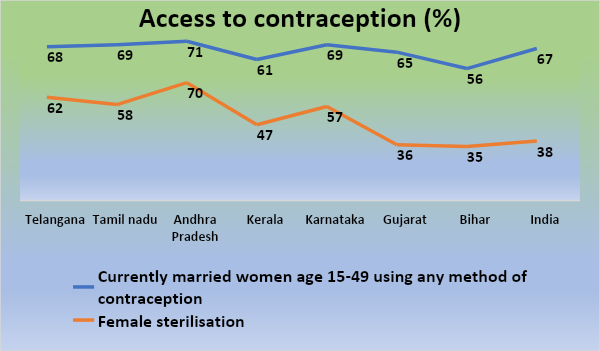
Access to contraception – NFHS 5. (Supplied)
According to the WHO, family planning is a fundamental health right that allows people to attain the desired number of children and determine pregnancy spacing. Further, this contributes to reducing pregnancy and abortion-related mortality and morbidity. Delaying pregnancy in younger women can positively affect their health and allow for more extended periods of education.
In India, currently, married women aged 15 -49 using any method of contraception is 67 percent.
The WHO says optimal feeding practices during infancy and early childhood include early initiation of breastfeeding, exclusive breastfeeding in the first six months of life, continued breastfeeding through age one year, timely introduction of complementary foods, diversity of diet, and frequency.
These are critical for child survival and development. In all states, not more than 67 percent (Kerala) have been fed within one hour of birth. The alarming increase in Caesarian sections can adversely affect the early initiation of breastfeeding (EIBF).
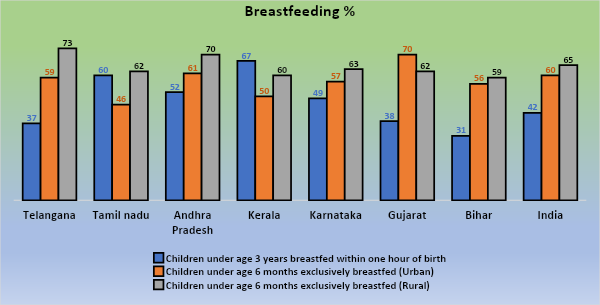
Breastfeeding percentage – NFHS 5. (Supplied)
Exclusive breastfeeding is the proportion of infants 0-5 months who received only breast milk during the previous day. Not more than 75 percent of children have been exclusively breastfed in rural areas.
Barriers to breastfeeding have to be addressed. Infants who are not breastfed are more at risk of malnutrition as well as respiratory and gastrointestinal infections, which are one of the largest contributors to infant mortality.
A nutritionally adequate diet in infants and young children ensures optimal growth, development, and health. Dietary diversity and adequate meal frequency can protect against several nutritional deficiencies and reduce morbidity and mortality in this vulnerable group.
The percentage of total children aged 6-23 months receiving an adequate diet (%) in India has gone up from 9.6 to a mere 11.3. This is dismal progress and calls for concerted nutritional interventions.
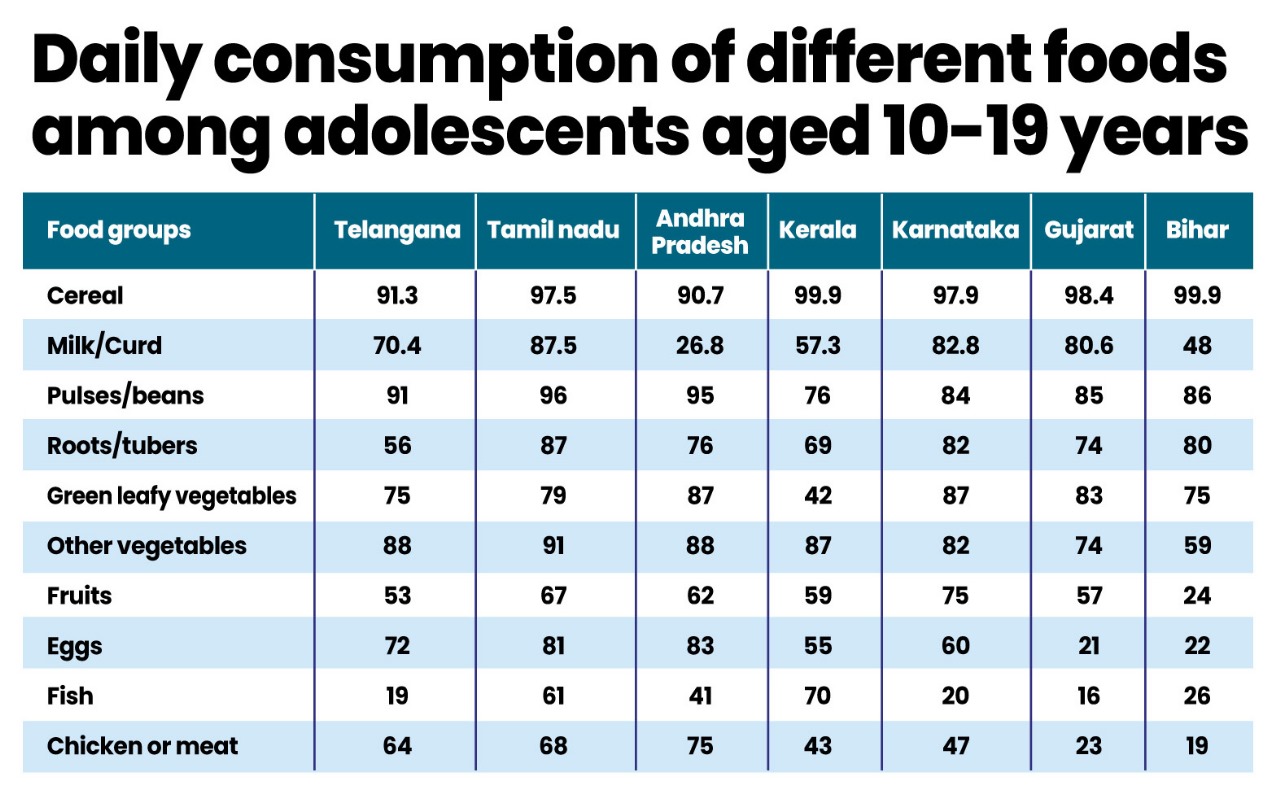
Daily consumption of different foods among adolescents aged 10-19 years.
The table (on the right) gives an overview of the kinds of foods eaten in different states (CNNS). A balanced diet should include foods from at least four of the six food groups — cereals and millets; legumes and pulses; eggs, poultry and fish; fruits and vegetables; fats and oils; milk and dairy.
Gujarat shows poor consumption of most animal-source foods (ASF) except milk, while Bihar has an overall low consumption of ASF, including milk. The consumption of milk or curd, fruits, eggs, fish or chicken, or meat was found to increase with higher levels of maternal schooling and household wealth (CNNS).
The percentage of children in India under 5 years who are stunted has come down from 38.4 to 35.5 percent between NFHS 4 and 5 and underweight from 35.8 to 32.1 percent.
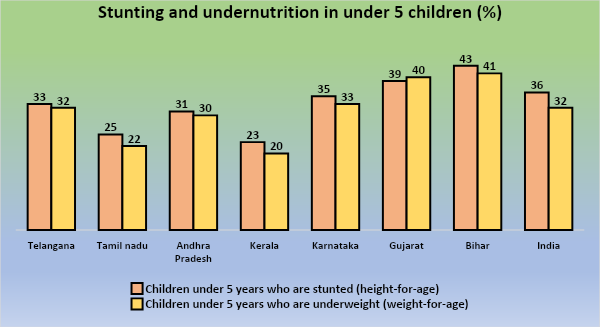
Stunting and undernutrition in children under 5 – NFHS 5. (Supplied)
Although anaemia is a well-known condition, it is often missed clinically and usually picked up in surveys. with classical signs of anaemia such as fatigue, breathlessness, etc., can be easily dismissed and only ‘managed’ with some painkillers and the generic advice to “eat properly”. Children with anaemia, especially those from marginalised communities, can often get labelled as ‘slow learners’ attributed more to their social backgrounds than their health.
There are many lessons to be learnt from Kerala’s multi-pronged approach to anemia being a low public health concern, however, there are pockets among tribal communities where anemia is a serious public health concern. This highlights the importance of breaking up the data even further when planning interventions.
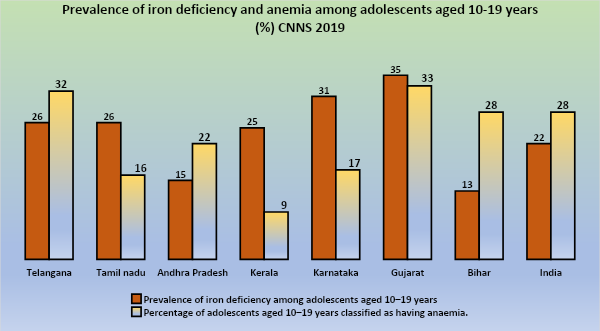
Prevalence of iron deficiency and anaemia among adolescents aged 10-15 years (%) – CNNS 2019. (Supplied)
Studies in South India have found associations between anaemia and livestock ownership, refined grain consumption, meat consumption, rurality, egg consumption, caste, etc. Repeated childbearing, lactation, and poor access to nutrition during menarche and pregnancy, as well as parasitic infections such as hookworm and malaria, may cause or exacerbate anaemia.
The multifactorial nature of anaemia aetiology can include deficiency of iron, folic acid, Vitamin B12, Vitamin A, riboflavin, pyridoxine, zinc, copper, etc. Understanding the prevalence of these nutrient deficiencies and improving diets are crucial rather than single nutrient interventions as currently being pushed in the form of fortification.
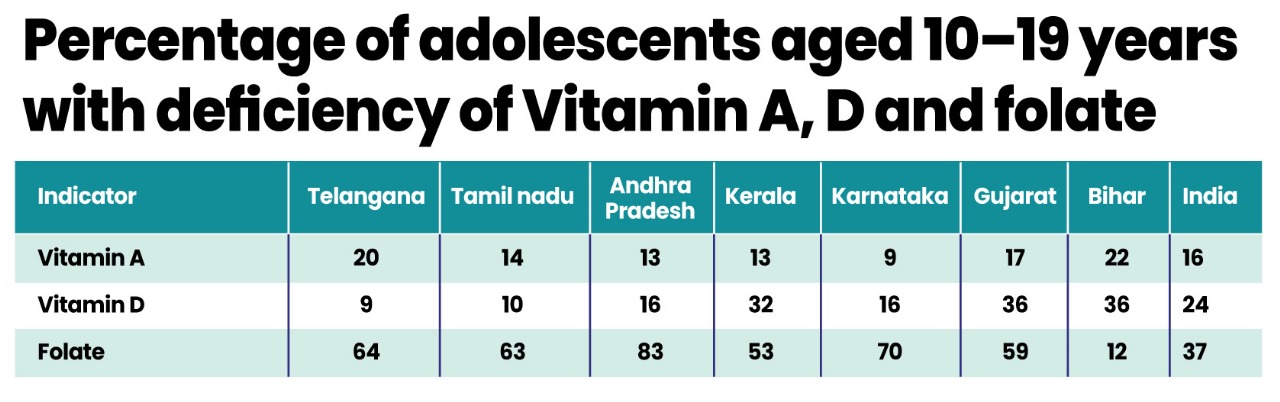
Percentage of adolescents aged 10–19 years with deficiency of Vitamin A, D and folate.
The table (to the left) shows the prevalence of deficiency of these important nutrients. These must be correlated with the other social determinants and diets to plan appropriate interventions.
Despite overall better performance in health indicators, the Southern States would do even better if they focused on social determinants, some of which have been highlighted here.
(The author is a public health doctor and researcher. Views are personal).
