Published Jan 06, 2024 | 8:00 AM ⚊ Updated Jan 06, 2024 | 8:00 AM


Currently, there are 19 Covid-positive cases admitted in ICUs across Karnataka. (Wikimedia Commons)

In a significant stride towards standardising intensive care practices across India, the Union Ministry of Health and Family Welfare recently unveiled comprehensive guidelines for Intensive Care Unit (ICU) admission and discharge.
Crafted in collaboration with leading experts from the Indian Society of Critical Care Medicine, these guidelines aim to establish clear criteria for the management of critical care units.
However, reactions from experts have been mixed, with some pointing out loopholes and confusions that the government may need to address for more straightforward implementation.

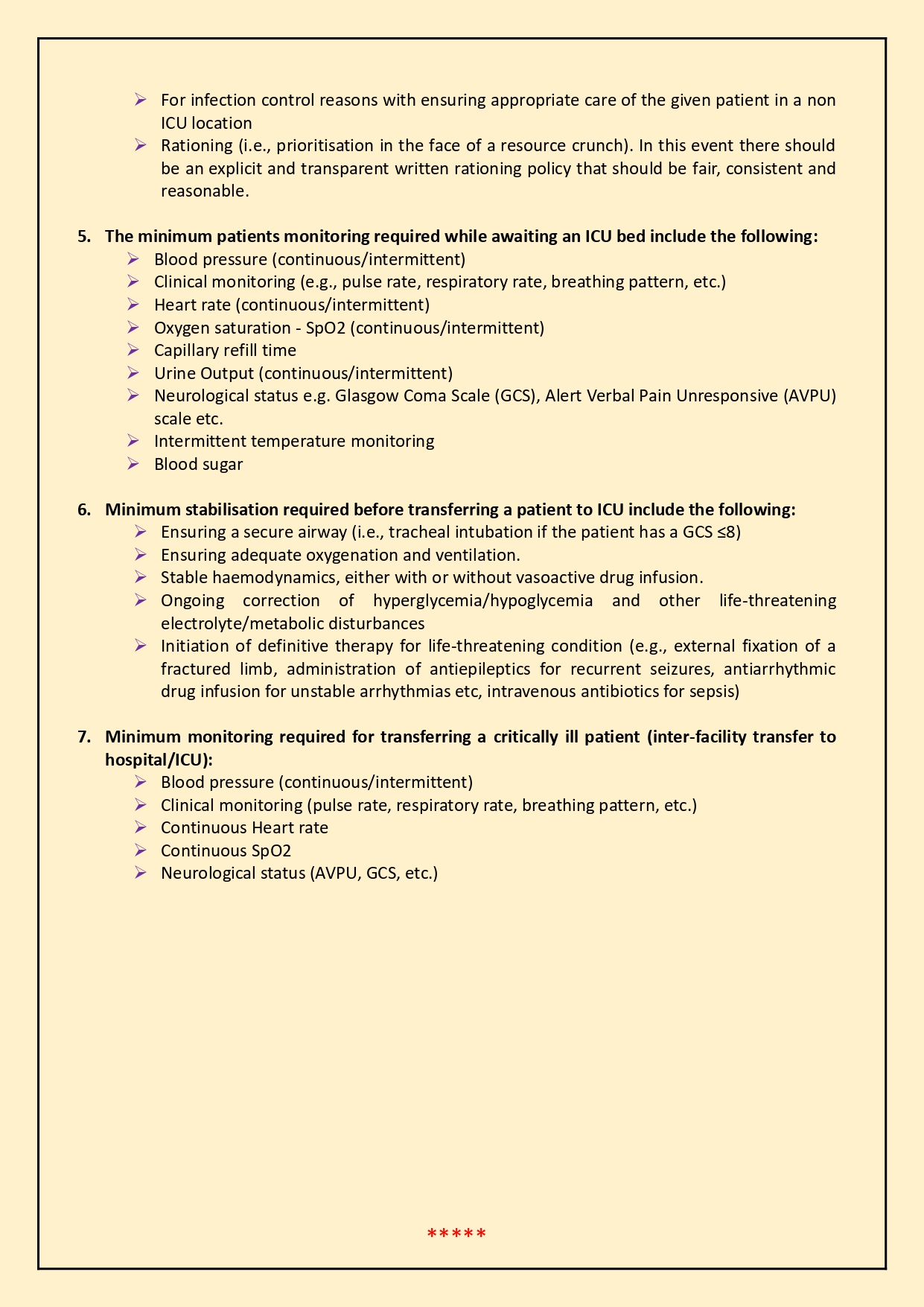
Guidelines for ICU admission and discharge criteria (Supplied)
The guidelines precisely define the role of an intensivist or critical care specialist (CCS), addressing a crucial need in the current healthcare landscape. Dr R Vijay Kumar, MD in General Medicine and Senior Physician at Hosmat Hospitals, commends this clarity, underscoring the inadequacy of ICUs managed by duty doctors without specialised training.
Furthermore, the guidelines state that MBBS doctors with three years of intensive care training are included as qualified intensivists. They also offer direction on the parameters qualifying a patient for ICU admission and specify who can make that call.
Concerning admission without consent, the guidelines assert, “A critically ill patient cannot be admitted to the ICU without the patient’s consent, or the consent of the family (if the patient is not in a position to give consent).”
Simultaneously, they also stipulate that individuals with an illness with a limited treatment plan or those with a living will (advance directive) against ICU care should not be admitted to the ICU.
As for discharge, the guidelines suggest that patients can be released when they achieve reasonable stability of the acute illness requiring ICU care or when the patient or their family agrees to ICU discharge. They also define who is authorised to make decisions on these matters, emphasising the requirement for a specialist overseeing the ICU to handle such calls.
Guidelines for ICU admission and discharge criteria (Supplied)
Dr Sunil Karanth, Chairman of Critical Services at Manipal Hospitals, Bengaluru, tells South First that these guidelines, developed with inputs from leading experts in the Indian Society of Critical Care Medicine, offer a comprehensive framework for the operation and management of intensive care units.
Dr Karanth explains that Critical Care Medicine, approximately three decades old and yet a relatively new specialty in India, lacks standardised definitions and guidelines. “These new policies will fill that gap, providing clear guidelines on the qualifications of an intensivist, the essential requirements of an ICU, and the patient admission criteria. This clarity will help remove ambiguities that previously existed in the understanding of ICU operations,” he says.
However, he emphasises that while the guidelines are a significant advancement, they should be adapted as needed and not misinterpreted as inflexible laws.
Despite their significance, these guidelines are not without challenges. Dr Karanth highlights a notable concern about the requirement for consent for ICU admission.
“In emergency situations, such as severe trauma cases, say in an accident case, if the patient has been brought to the hospital by a good Samaritan, and is in a critical condition, obtaining consent might be impractical, potentially delaying critical care,” he explains.
Meanwhile, Dr Harish MM, Intensive Care Physician and Infectious Disease Specialist, Director of Institute of Critical Care Medicine at Kauvery Hospitals in Bengaluru, tells South First, “The guidelines do not explicitly address the rights of intensivists regarding independent admission under critical care teams.”
One immediate concern highlighted by Dr Vijay Kumar is the current state of ICU management in smaller hospitals, where intensivists are often unavailable. “These ICUs are typically overseen by duty doctors, relying heavily on telephonic consultations with consultants,” he explains to South First.
This set-up, Dr Kumar points out, is inadequate due to the specialised knowledge and skills required for ICU care.
In such situations, the new guidelines, by setting higher standards for ICU management, raise important questions: Do these guidelines also mean that small and medium-sized hospitals should close their ICUs? Will they cripple the already existing critical care setup amidst an acute shortage of ICUs in the country?
Dr Kumar argues that, on a positive note, the guidelines recognise MBBS doctors with a three-year intensive care certificate course as qualified to serve as intensivists, broadening the pool of eligible professionals.
This inclusion, he notes, is a welcome move, particularly for enhancing critical care in regions with limited access to traditionally qualified specialists.
However, he also points out a concerning ambiguity, “The same guidelines have a weak clause, stating that an MBBS doctor without a postgraduate degree or a Indian Society Of Critical Care Medicine qualification can also work as an intensivist, provided they have extensive work experience in the ICU with >50 percent time spent in the ICU.”
“In such cases, who will certify these doctors and how will one quantify or measure time spent in the ICU? These are the questions that have no answers,” rues Dr Kumar.
Furthermore, the guidelines’ decision to exclude AYUSH doctors from being recognised as intensivists is seen as a significant and necessary distinction by many doctors.
However, speaking to South First, Dr Kiran Madhala, Convenor of the Indian Medical Association and Head of Department at the Critical Care Department, Nizamabad Government Medical College, says, “The specialists mentioned as critical care experts are fewer in number. They need to add more experts from departments like Anaesthesiology, Respiratory Medicine, and General Medicine to the list of critical care experts.”
Further, “ICU admission or discharge criteria doesn’t clearly mention conditions; it is purely the treating physician’s decision,” he says and adds that the admission criteria mentioned is confusing and not patient-friendly.
Doctors explain that there might be conflict when the family of a terminally ill patient wants them admitted in the ICU, while the guidelines states that patients who are terminally ill with a medical judgement of futility need not be admitted to ICU.
Meanwhile, Dr Kumar says that the new guidelines also define who should not be admitted to ICU. “One who has a living will against ICU care is a new thought by the government. Whereas, other criteria like refusal by patient to admit in ICU and terminally ill patients with high mortality are already widely practiced in most hospitals, with written consent of close relatives,” he says.
On the topic of discharge criteria, Dr Kumar highlights the added responsibilities for doctors, “One of the discharge criteria has put an additional responsibility on the treating doctor, which states that lack of benefit from aggressive care can prompt an Intensivist to shift a patient out of the ICU. This should always be with full written consent of the close relatives/caretakers of the patient.”
Most of the guidelines, organised under seven headings, align with practices already common in many hospitals, indicating a move towards standardisation rather than revolution in ICU management.
