Published Jul 15, 2026 | 7:00 AM ⚊ Updated Jul 15, 2026 | 7:00 AM


AD350 drone used for sputum transport; the red box highlights the secure storage compartment with a protective lid.

Synopsis: A study by AIIMS Bibinagar found that transporting tuberculosis sputum samples by drone instead of requiring patients to travel cut the average cost of diagnosis by nearly 99 percent in rural Telangana. The programme also reduced the median time from a patient’s first visit to diagnosis from 15 days to five by flying samples from remote health centres to TB testing facilities.
Spread across 3,253 sq km, Yadadri-Bhuvanagiri is one of Telangana’s largest districts. Much of its population of 770,833, according to the 2011 Census, lives in villages scattered across hilly terrain, where poor roads and limited public transport make healthcare difficult to access.
For people suspected of having tuberculosis (TB), getting tested usually means travelling 10 km to 30 km to the nearest TB Unit equipped with GeneXpert or Truenat machines. Primary Health Centres and sub-centres closer to their homes do not have molecular diagnostic facilities.
For many patients, the journey takes an entire day and comes with steep out-of-pocket expenses.
A study by the All India Institute of Medical Sciences (AIIMS) Bibinagar found that transporting sputum samples by drone instead of asking patients to travel reduced the average out-of-pocket cost of TB diagnosis from ₹9,451 to ₹90.9, a decline of nearly 99 percent.
“This study evaluated the impact of integrating drone-based sputum transport into the TB diagnostic network in the rural Yadadri-Bhuvanagiri district of Telangana, India. To our knowledge, this is the first programme-based study conducted in collaboration with the National TB Elimination Programme (NTEP) of India that assessed drone transport over an extended duration,” the authors wrote.
The study, conducted under the Indian Council of Medical Research’s i-DRONE initiative in collaboration with the National TB Elimination Programme, compared the conventional road-based system with drone transport.
It found that flying sputum samples to diagnostic centres, rather than requiring patients to make the trip themselves, sharply reduced the financial burden of accessing TB testing in remote communities.
Also Read: Food first, supplements only when needed, says Endocrine Society of India’s first calcium guidance
The researchers selected four TB Units (TUs), 11 Primary Health Centres (PHCs) and 60 sub-centres across Yadadri-Bhuvanagiri, choosing sites with a high TB burden, poor connectivity and no molecular diagnostic facilities.
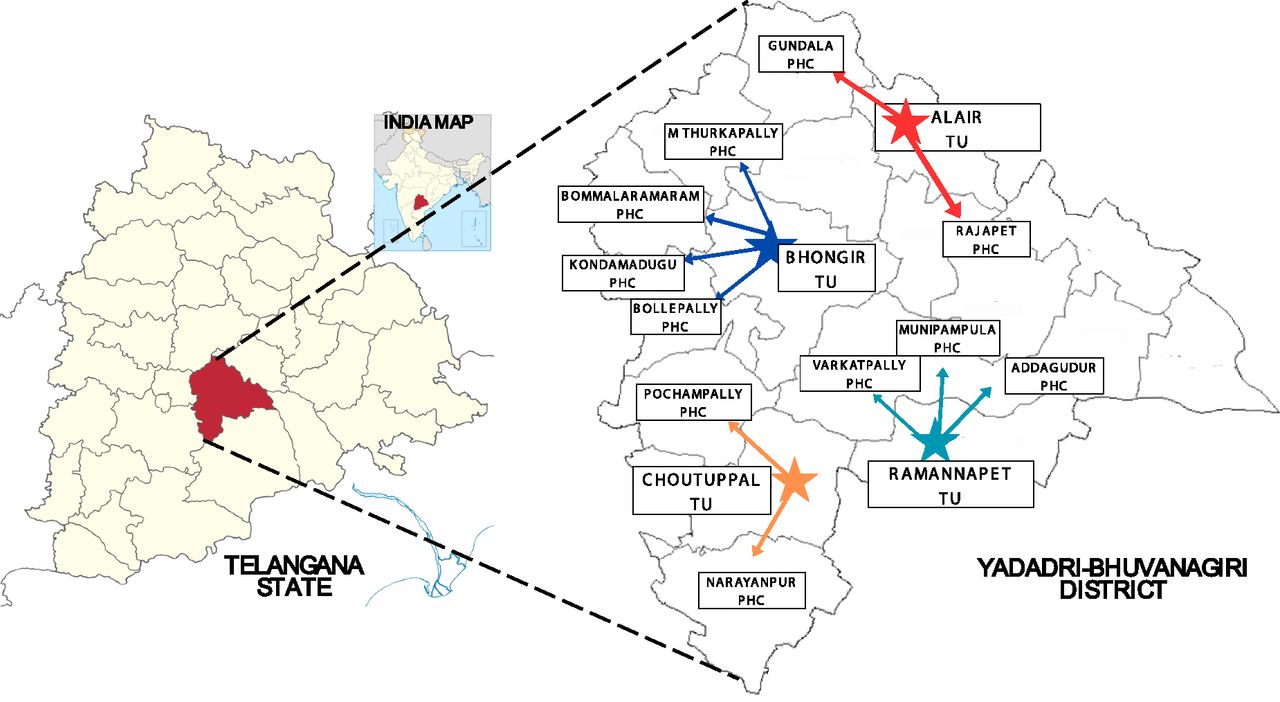
The map illustrates the operational flow from the central command centre at AIIMS Bibinagar to the District TB Centre, and PHCs_Kamble, B. Ganji et al
They compared patient costs during a pre-drone phase (February-December 2023) with those recorded after drone operations began (February 2024-February 2025). The study enrolled 206 TB patients before the intervention and 634 people with presumptive TB afterwards.
The researchers calculated out-of-pocket expenditure using three components: direct medical costs, including consultation, medication and diagnostic tests; non-medical expenses such as travel and food; and indirect costs, largely wages lost by patients and the family members accompanying them. By eliminating the need for patients to travel to TB Units for testing, drone transport removed much of this financial burden in one step.
While average out-of-pocket expenditure fell by nearly 99 percent, the median expenditure during the drone phase dropped to zero, reflecting the fact that most patients either walked to their nearest PHC or spent no more than ₹50 on local transport.
Direct medical costs fell from ₹7,017 to ₹75.8, non-medical expenses from ₹787 to ₹12.4, and indirect costs from ₹1,646 to ₹2.71. All three reductions were statistically significant, with P values below 0.001.
“A 99% reduction in out-of-pocket expenditure in our study further underscores the economic benefit of drone-enabled sputum transport,” the authors wrote.
The intervention also sharply reduced the time taken to diagnose patients.
The median turnaround time from a patient’s first visit to a health facility to diagnosis fell from 15 days to five, while the mean dropped from 16.6 days to 6.9 days.
Reporting times improved even more dramatically. Before drones were introduced, 92.2 percent of patients waited more than two days for their test results. During the drone phase, that share fell to 16.3 percent. More than three-fourths of patients (76.3 percent) received their results the next day, up from just 1.5 percent before the intervention. Same-day reporting changed little, rising from 6.3 percent to 7.4 percent.
The researchers also recorded a steep decline in diagnostic delay, the interval between a patient’s first contact with a health worker and confirmation of TB. The median fell from 15 days to six, while the mean dropped from 17.6 days to 7.9 days.
Patient delay, by contrast, changed little. The median time between the onset of symptoms and a patient’s first contact with the health system remained at six days in both phases. The mean, however, fell from 16.6 days to 9.2 days, suggesting there were fewer patients with exceptionally long delays in seeking care after the intervention.
“The intervention was associated with significant reductions in turnaround time, diagnostic delays, patient delays and out-of-pocket expenditure, highlighting the potential of drone logistics to enhance equitable access to TB care in India,” the researchers wrote.
The drone network is coordinated from a command centre at AIIMS Bibinagar, where a licensed pilot oversees flight operations and monitors missions in real time.
The system follows a hub-and-spoke model. Primary Health Centres (PHCs) and sub-centres collect sputum samples, while four TB Units equipped with CBNAAT or Truenat machines serve as diagnostic hubs.
After a patient provides a sputum sample at the nearest PHC or sub-centre, health workers seal it in triple-layer packaging that complies with the Indian Council of Medical Research’s biosafety protocol for drone transport before dispatching it to a TB Unit.
The programme uses two drone models: the AD250, which weighs 11.5 kg and can carry up to 2 kg of cargo, and the larger AD350, which weighs 24 kg and has an 8 kg payload capacity.
Flights follow pre-programmed routes based on Keyhole Markup Language (KML) files that take into account terrain, population density and no-fly zones. Teams also identified dedicated take-off and landing sites at all 75 participating health facilities in accordance with the Drone Rules, 2021, selecting locations that balanced proximity to the facilities with operational requirements.
Also Read: The calcium paradox: Why the mineral your bones need doesn’t necessarily damage your heart
The researchers found that the drone programme reached a different patient population than the conventional system, extending diagnostic access into some of the district’s most underserved communities.
Participants enrolled during the drone phase were, on average, older, less educated and poorer than those in the pre-drone phase. The mean age rose from 49.1 years to 59.8 years, while the share of patients with no formal education increased from 47.1 percent to 80.4 percent.
More than 80 percent of participants in both phases lived below the poverty line. During the drone phase, 91.3 percent reported a monthly income of less than ₹5,000, compared with 71.4 percent before the intervention. A cough lasting more than two weeks remained the most common symptom in both groups.
The researchers said this shift most likely reflected the programme’s expansion into remote areas rather than any change in the epidemiology of TB. At the same time, they cautioned that the demographic differences should be taken into account when comparing outcomes across the two phases, as older, poorer and less educated populations may face barriers to care that extend beyond transport.
“During the drone phase, participants were generally older, less educated and economically disadvantaged. While this likely reflects the operational expansion of the intervention and improved diagnostic reach among underserved communities, it also needs to be considered when interpreting comparative outcomes,” the authors wrote.
The authors describe the project as the first programme-based study conducted with India’s National TB Elimination Programme (NTEP) to evaluate drone transport over an extended period.
They attribute the sharp reduction in out-of-pocket expenditure primarily to eliminating the need for patients to travel to diagnostic centres, arguing that the findings highlight the economic value of drone-enabled sputum transport in settings where the cost of seeking care remains a major barrier.
The researchers also situate their findings within a growing body of evidence on the use of drones in public health. Studies from Uttarakhand and northeast India have shown that drone transport can shorten diagnostic delays in difficult terrain, while programmes in Ghana found aerial vaccine delivery to be cost-effective, with incremental cost-effectiveness ratios as low as USD 41 per disability-adjusted life year averted. In Malawi, a similar unmanned aerial vehicle (UAV) programme reduced turnaround time for early infant HIV diagnosis, and in Manipur and Nagaland, drones delivered more than 20,000 medical supplies despite challenging geography.
“This is the first programme-based study conducted in collaboration with the NTEP of India that assessed drone transport over an extended duration,” the authors wrote.
“A 99% reduction in out-of-pocket expenditure in our study further underscores the economic benefit of drone-enabled sputum transport,” they added.
The authors caution that the findings should be interpreted in light of several limitations. The study compared outcomes before and after the intervention but did not include a concurrent control group, making it difficult to attribute all of the observed improvements solely to drone transport.
Patient expenditure was based on self-reported estimates, leaving room for recall bias. The relatively short study period also meant the researchers could not determine whether faster diagnosis ultimately improved treatment initiation, adherence or longer-term health outcomes.
They further noted that participants enrolled during the drone phase were older, poorer and less educated than those in the pre-drone phase. Those differences may have influenced some of the observed outcomes and should be considered when comparing the two groups.
Even so, the authors argue that the findings support expanding the model to improve access to TB diagnosis in underserved communities.
“The intervention showed reductions in turnaround time, delays and out-of-pocket expenditure, benefiting the vulnerable population,” they wrote, adding that such approaches could help India move closer to eliminating TB.
