Published Jun 20, 2025 | 1:48 PM ⚊ Updated Jun 20, 2025 | 1:48 PM


Neighboring states like Tamil Nadu and Karnataka have already made snakebite notifiable disease. Why, then, is Kerala still lagging behind? (IMG- roundglasssustain.com)
Synopsis: Despite snakebites causing more deaths than elephant attacks in Kerala – 598 fatalities over the past decade – the state has yet to declare it a notifiable disease, unlike its neighbours Tamil Nadu and Karnataka. Experts argue that mandatory reporting would enable better data collection, hospital preparedness, and ultimately, save lives across the state.
Imagine bidding goodbye to your daughter in the morning, trusting she was safe at school – only to find yourself, shattered, standing outside a mortuary by evening, waiting to receive her lifeless body.
In Wayanad’s Sulthan Bathery, advocates Abdul Azees and Sajna Ayisha know exactly how that feels.
On a tragic day in November 2019, their daughter, Shahla Sherin, a 10-year-old Class V student, left for school as bubbly as ever. But at the Sarwajan Vocational Higher Secondary School in Sulthan Bathery, a venomous snake bit her inside her classroom. Shahla did not survive.
Multiple versions of the incident circulated as public anger – though short-lived – flared against the school and the alleged negligence in ensuring a safe environment for children.

Shahla Sherin
One version suggested that the snake, believed to be a viper, slithered into the classroom and bit the girl’s leg around 3.10 p.m. Another claimed it had been coiled inside a crack in the classroom wall, and Shahla’s leg got caught in the crevice.
The classroom itself was in poor condition – hardly a space where children should be expected to learn. A delay in transporting Shahla to a hospital for antivenom treatment ultimately sealed her fate.
Regardless of the events, the outcome was the same. Shahla Sherin, who had left home full of life that morning, was brought back still, cold, and covered in a shroud. It was a tragedy that should never have occurred in a place considered safe for children.
India – once viewed by outsiders as the land of snake charmers and decorated elephants – has, since 2011, earned the sobering distinction of being the snakebite capital of the world. The country accounts for nearly half of all global snakebite cases, with over 55,000 deaths each year.
In Kerala, the Department of Forest and Wildlife has taken a number of effective steps to reduce such fatalities. However, a key measure remains pending nearly six years since Shahla Sherin’s untimely death: the classification of snakebite as a notifiable disease.
Neighbouring Tamil Nadu and Karnataka have already taken this step. Why, then, is Kerala still lagging behind?
Snakebite has been officially recognised as a notifiable disease in India, following a directive from the Union Ministry of Health and Family Welfare.
Punya Salila Srivastava, Secretary in the Ministry of Health & Family Welfare, in a circular last November, instructed all states and union territories to report snakebite cases under the Integrated Disease Surveillance Programme (IDSP).
To coordinate and implement this directive, the National Centre for Disease Control (NCDC) appointed Dr Ajit Shewale, Joint Director, as the National Nodal Officer.
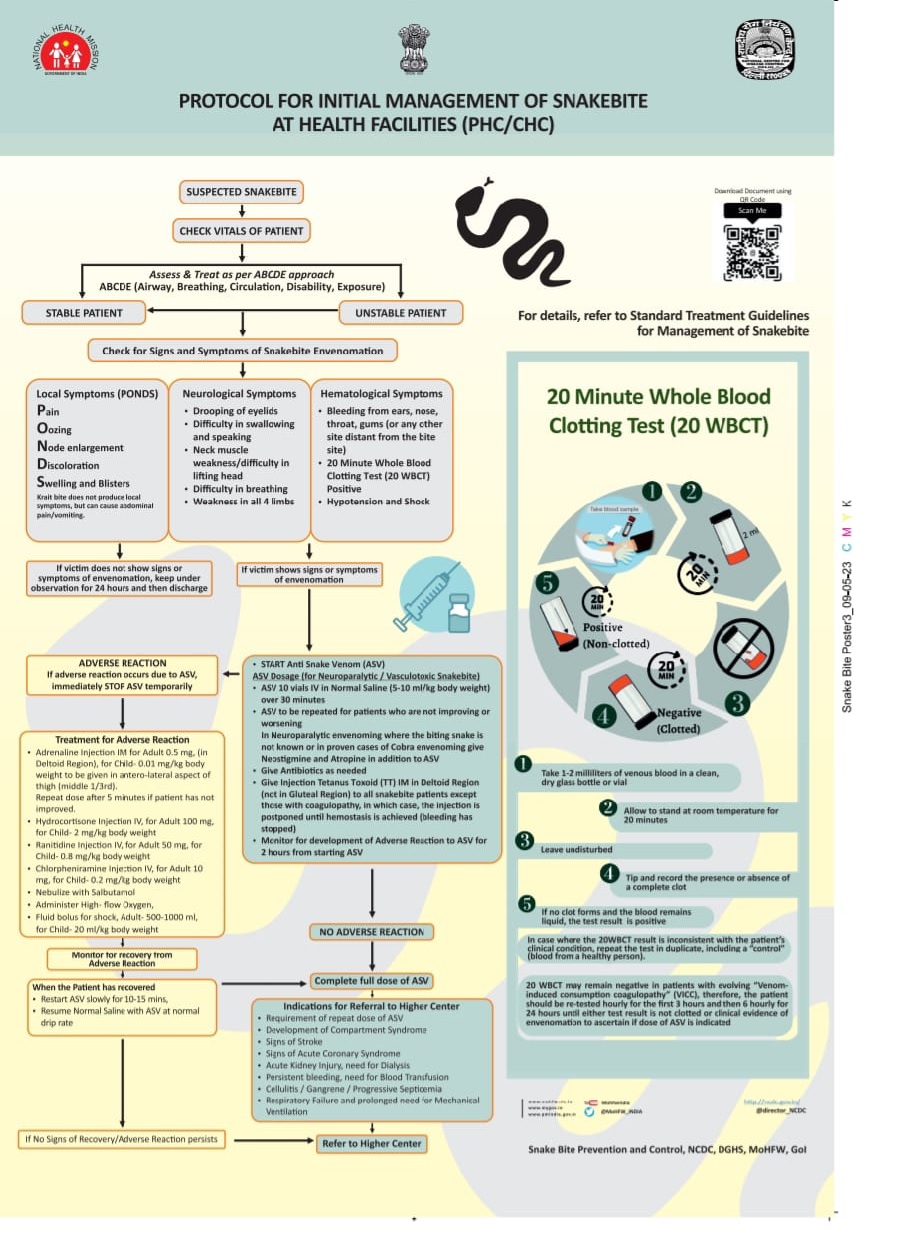
Protocol for initial management of snakebite at PHC/CHC
The move aligns with the World Health Organization’s goal of reducing global snakebite deaths by 50 percent by 2030. In line with this, India launched the National Action Plan for Prevention and Control of Snakebite Envenoming (NAPSE).
Meanwhile, earlier this month, the Kerala High Court also made strong observations supporting this initiative.
In a joint judgment in WPC Nos. 32493/2019 and 34037/2019, on 5 June, a bench comprising Justices Nitin Jamdar and Shoba Annamma Eapen emphasised the importance of declaring snakebite a notifiable disease.
Several states, including Odisha (20.12.2024), Tamil Nadu (04.11.2024), and Karnataka (12.02.2024), have already issued notifications. Kerala, however, has yet to take formal action, although a proposal is reportedly under active consideration by the government.
The inaction is especially concerning, since between 2016–17 and 2025–26, Kerala recorded a total of 598 human deaths due to snakebites, making it the leading cause of fatalities among all human–wildlife conflict incidents, according to data from the Kerala Forest Department.
Snakebite deaths were especially high in the initial years: 75 in 2016–17, 92 in 2017–18, and peaking at 123 in 2018–19.
That peak alone accounted for over 20 percent of all such deaths during the decade. The toll was 71 in 2019–20, followed by 52 in 2020–21 and 65 in 2021–22.
Notably, the trend showed a steady decline in recent years, with 48 deaths in 2022–23, 34 each in 2023–24 and 2024–25, and only 4 in 2025–26.
By comparison, elephant attacks – the second leading cause – claimed 205 lives over the same period, with the highest annual toll of 35 recorded in 2021–22. Fatalities due to wild pigs (58), gaurs (10), tigers (10), and others (15) remained significantly lower.
Interestingly, wasp and bee stings have risen sharply toward the end of the decade, accounting for a total of 54 deaths – including 18 in 2023–24 and 23 in 2024–25.
Nevertheless, snakebite continues to be the single largest cause of human deaths in wildlife conflict cases, and needs to be treated as a public health crisis in Kerala.
Post Shahla Sherin’s death, her family has not taken legal action against the school or hospital authorities.
Yet, the Kerala High Court took up the matter suo motu, and the recent discussions on designating snakebite as a notifiable disease were linked to Shahla’s case.
“The school building was renovated, and they promised to name it after my daughter – but I don’t know when that will happen. Everything – the case, the reports, the inquiries – is moving so slowly. My daughter could’ve been saved if she had been taken to a better hospital on time,” Shahla’s father, Advocate Abdul Azees, told South First.
The family received ₹10 lakh from the state government, ₹2 lakh from the Forest Department, and ₹50,000 from the Education Department as compensation.

The new school building
Shahla was bitten by a venomous snake inside her classroom at around 3.15 p.m., but she was only taken to a hospital with antivenom by 6.30 p.m. By then, the venom had spread through her body, and she died.
Though Shahla and her classmates reportedly told their teachers that it was a snakebite, they allegedly delayed seeking medical help – triggering public outrage.
A case was later filed against Taluk Hospital doctor Jisa, headmaster Mohankumar, principal Karunakaran, and teacher Shijil.
The incident drew widespread attention after Shahla’s friends revealed that they had spotted a snake in the area earlier and warned the teachers – warnings that were allegedly ignored. That inaction cost a life.
Health experts explain that a notifiable disease is one that must, by law, be reported to public health authorities – not just as an administrative requirement, but as a critical measure to protect public health.
The state Health Department has submitted a proposal to declare snakebite a notifiable disease, but it was still awaiting approval.
“The biggest advantage of making snakebite a notifiable disease is that all related data can be compiled on a single online portal. This would help us analyse trends – such as seasons, species involved, vulnerable regions, and timings – giving us a clear picture of snakebite risk across the state,” Assistant Conservator of Forest Muhammad Anvar Yunus told South First.
Anvar also stressed the importance of improving hospital preparedness.
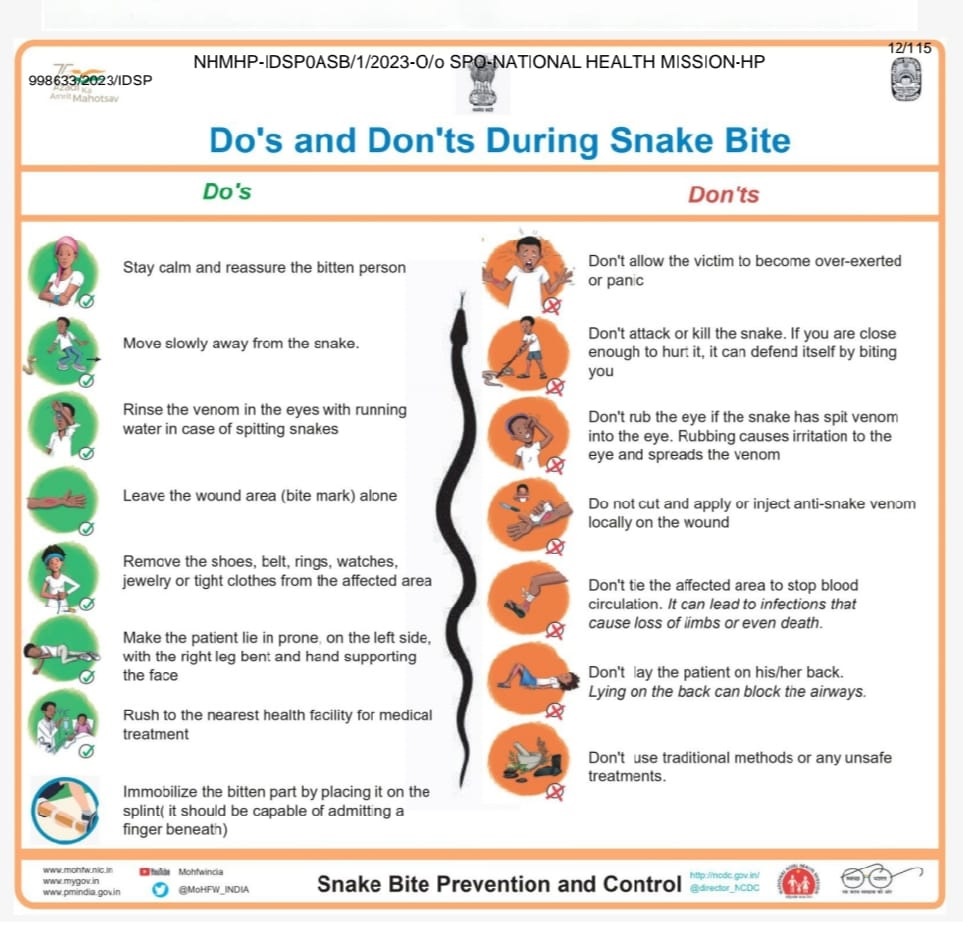
Do’s and Dont’s during Snake bite
“Taluk hospitals must be equipped to identify whether a bite is venomous. Only then can we reduce fatalities. Referring every case to a district medical college increases the risk. Many PHCs do not have doctors available after noon. If we miss the golden hour, a life could be lost. At the very least, minimum treatment must be ensured at the PHC level,” he added.
He further noted that the Forest Department had increased the compensation for snakebite deaths from ₹2 lakh to ₹4 lakh. The revised amount applies to deaths occurring on or after 7 March 2024.
However, the disbursement process has not yet begun, as procedural formalities are still underway.
According to the protocol for initial management of snakebite at PHC and CHC-level health facilities, patients must be assessed using the ABCDE approach (Airway, Breathing, Circulation, Disability, Exposure) and checked for signs of envenomation.
Based on the patient’s clinical stability and symptoms – local, neurological, or haematological – treatment with Anti-Snake Venom (ASV) may be initiated.
The 20-minute Whole Blood Clotting Test (20 WBCT) is a key diagnostic tool used to detect coagulopathy.
The protocol also outlines how to manage adverse reactions and the criteria for referral to higher centres, ensuring timely and standardised care.
The Directorate of the State Health Department has recently submitted a detailed report to the Kerala High Court in response to its query on measures taken to prevent snakebite deaths, as part of the suo motu case relating to the Wayanad student’s death.
It was the court that noted snakebite cases would soon be declared a notifiable disease. The state government, however, cited Kerala’s robust health infrastructure and geographical proximity to healthcare facilities, arguing that there was no need to rush, and that no significant delay existed at the state level.
Dr Ajan MJ, Assistant Director at the Health & Family Welfare Department, told South First that a comprehensive report had already been submitted to the government recommending that snakebites be made a notifiable disease.
“Even though Kerala is better in treatment, we lack clarity – especially regarding cases treated in private hospitals. Although animal bite diseases are supposed to be mandatorily reported, some still go unreported – even if the numbers are small,” he said.
However, officials acknowledged that accurate reporting must begin at the Primary Health Centre (PHC) level to ensure full data coverage. In contrast, the Forest Department maintains a near-complete record of snakebite deaths, as they are linked to compensation claims.
In Kerala, heavy rains and flooding during the monsoon season often drive snakes – some venomous – into homes, posing serious risks to residents. To address this, the Forest Department launched the SARPA app (Snake Awareness, Rescue, and Protection App) in January 2021, in collaboration with the Wildlife Trust of India.

Snakebite coordinators inspected St. Mary’s UP School, Vandur, under the Chalakudy Social forestry division.
The app enables people to quickly connect with trained snake rescuers. There are over 1,720 such professionals and volunteers across the state, including more than 200 trained women.
Assistant Conservator of Forests Muhammad Anvar Yunus told South First that strict protocols are followed in handling snakes. Actor Tovino Thomas, as the app’s brand ambassador, helped significantly raise public awareness.
Notably, Palakkad district – once among the first in the state to report snakebite cases – has seen a significant drop in recent years, attributed in part to improved awareness and coordinated rescue efforts.
The most recent state budget proposal to achieve zero mortality from snakebites within five years marks the final phase of an ambitious campaign launched in recent years. The state also plans to establish an anti-venom production facility to support this goal. The finance minister announced that the Snake Envenomation Zero Mortality Kerala initiative will be implemented state-wide.
As the rains return to Kerala and schools reopen, SARPA teams are conducting safety checks and awareness programmes in schools as part of reopening efforts. These steps are vital to ensure that no life is lost and no home is silenced again – like Shahla’s.
(Edited by Dese Gowda)
