
Published Mar 24, 2026 | 7:00 AM ⚊ Updated Mar 24, 2026 | 9:39 AM

")
Tuberculosis. (iStock)
Synopsis: In Tamil Nadu, the programme records note that the state currently has 461 TB Units, 1,951 Designated Microscopy Centres and more than 450 NAAT laboratories for molecular testing. This network enables the detection and diagnosis of both drug-sensitive and drug-resistant TB, while trained specialists in TB and chest diseases serve as District TB Officers and oversee implementation at district TB centres, ensuring the availability of medicines, diagnostics and patient follow-up services.
At the diagnostic centre inside the Government Hospital of Thoracic Medicine, popularly known as the Tambaram TB Sanatorium, patients sit quietly on benches waiting for their turn.
Some have come with persistent cough and breathing trouble, while others are admitted for observation as doctors try to determine whether their symptoms are caused by tuberculosis or another lung condition.
During a visit by South First, patients could be seen moving between the diagnostic centre and wards for tests and observation.
Inside the wards, families waited anxiously as doctors carried out multiple tests before confirming what exactly was causing a patient’s breathing problems.
The hospital, one of the state’s key tuberculosis care facilities, sees a steady flow of patients undergoing tests and monitoring every day.
When South First met Revathi, a caretaker of a patient with a history of smoking admitted there, she said doctors had advised several tests to determine the exact cause of his breathing problem, including a routine screening for tuberculosis — a step often taken in patients considered to be at higher risk.
“They told us the results look normal, but they are doing some more tests to find out what the problem is. So they asked him to stay here for observation,” Revathi said.
The waiting period has been difficult for the family.
“It has already been three days since he was admitted. We are still waiting for the final reports, and the doctors have not told us yet when he can be discharged,” she added.
While the uncertainty weighs heavily on families, the process also reflects how patients with lung symptoms are carefully screened and diagnosed before doctors conclude.
Another caretaker at the hospital pointed to a challenge doctors often face when patients migrate for work.
“Many people in our area go to other cities for work. If someone starts treatment here and then has to leave for a job, it becomes very difficult to continue the medicines regularly. Some people stop halfway because they cannot keep travelling back to the hospital,” said Kumar to South First, who was accompanying his father.
India continues to carry one of the world’s largest tuberculosis burdens, accounting for nearly 26 percent of global TB cases, according to the National Tuberculosis Elimination Programme (NTEP).
In Tamil Nadu, the programme records note that the state currently has 461 TB Units, 1,951 Designated Microscopy Centres and more than 450 NAAT laboratories for molecular testing.
This network enables the detection and diagnosis of both drug-sensitive and drug-resistant TB, while trained specialists in TB and chest diseases serve as District TB Officers and oversee implementation at district TB centres, ensuring the availability of medicines, diagnostics and patient follow-up services.
Tamil Nadu was also the first state to conduct a district-level TB prevalence survey to better understand differences in disease burden across districts.
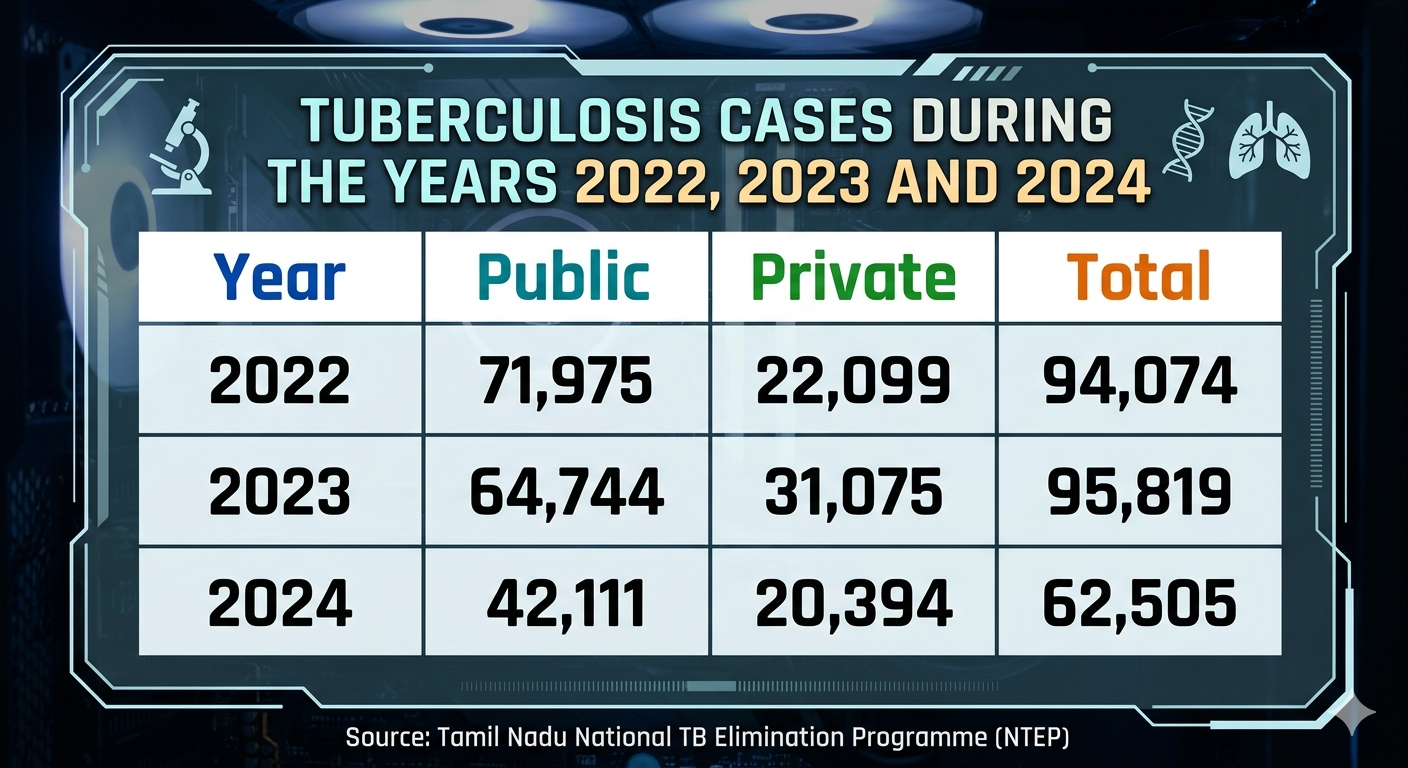
Tuberculosis cases.
Between 2022 and 2024 (January–August), Tamil Nadu saw a gradual decline in public sector TB notifications—from 71,975 cases in 2022 to 42,111 in early 2024—while the private sector’s role grew, rising from 22,099 cases in 2022 to 31,075 in 2023 before slightly dipping to 20,394 in 2024.
Overall, total TB notifications increased slightly in 2023 compared to 2022 and remained strong at 62,505 in the first eight months of 2024, reflecting a shift toward stronger engagement from private providers in detecting and reporting cases.
As of the second quarter of 2024, Tamil Nadu recorded a TB case notification rate of 124 per 100,000 population, while the treatment success rate stood at 85 percent, reflecting improvements in timely diagnosis and treatment.
Private healthcare providers are also playing a growing role in TB detection and reporting. According to programme records, TB notifications from the private sector increased from 44 percent in 2017 to 89 percent by mid-2024, indicating stronger collaboration between public and private healthcare systems.
Diagnostic capacity has also expanded with the implementation of Universal Drug Sensitivity Testing (UDST), under which 94 percent of microbiologically confirmed TB patients are tested for drug resistance. This helps doctors tailor treatment regimens and prevent the spread of resistant strains.
Despite progress, challenges remain — particularly in addressing drug-resistant tuberculosis (DR-TB).
Programme data shows that during the second quarter of 2024, 8,503 presumptive DR-TB cases were tested, resulting in the identification of 637 drug-resistant TB patients.
Treatment success rates for DR-TB have improved to over 70 percent, though continued efforts are needed to strengthen diagnostics, treatment, and patient support.
Tamil Nadu has introduced new strategies to strengthen TB care, including “Kasa Noi Erapilla Thittam”, a model that screens for severe illness at diagnosis and provides inpatient care when needed.
Other measures, such as mobile diagnostic units and shorter TB preventive treatment regimens launched in 2023, aim to improve early detection and treatment adherence.
Tuberculosis treatment.
A senior government doctor working in Tamil Nadu’s state TB programme, speaking to South First on condition of anonymity, highlighted the patterns he often sees among patients.
“Pulmonary TB usually shows as a cough for over two weeks, chest pain, or blood in sputum,” he said, adding, “Other symptoms include fatigue, weight loss, fever, or night sweats. Symptoms differ if TB affects other organs.”
He noted that delayed presentations are common. “Many patients first try home remedies or self-medication before coming to a health facility. Social stigma around TB also discourages people from accepting the diagnosis early,” he observed.
Around one in five extra-pulmonary cases in high-burden areas is diagnosed clinically, without microbiological confirmation, which adds to the complexity.
Despite these challenges, the public system enables rapid treatment initiation.
“Once diagnosed in government centres, patients typically start therapy within a week with free anti-TB drugs under the National TB Elimination Program. Yet, issues like high pill burden, treatment duration of six months or more, and adherence difficulties remain significant,” he noted.
He also highlighted that private referrals often lead patients to public care only after initial delays or costs in the private sector.
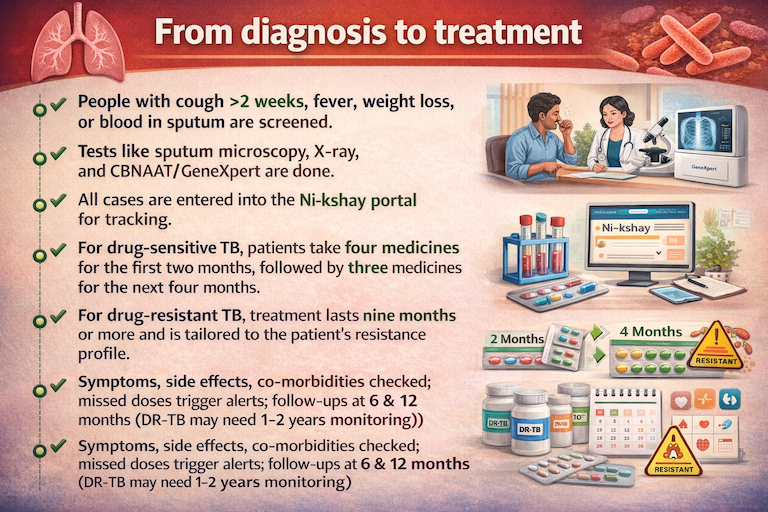
Patients with a cough lasting more than two weeks, fever, weight loss, or blood in sputum are screened carefully.
“We use sputum microscopy, chest X-rays, and rapid molecular tests like CBNAAT or GeneXpert to confirm TB. Every confirmed case is entered into the Ni-kshay portal, so patients can be tracked and none are lost in the system,” the doctor said.
“For drug-sensitive TB, treatment starts with four medicines for two months, followed by three medicines for four months,” he explained.
“It’s daily and free at government hospitals. For drug-resistant TB, the regimen is longer—nine months or more—and tailored to the patient’s resistance profile.”
Monitoring is continuous, he noted.
“At follow-ups, we check symptoms like cough, fever, and weight loss, and watch for side effects such as liver issues, rashes, neuropathy, or vision and hearing changes. We also manage co-morbidities like diabetes or HIV. Drug-resistant patients get extra tests, including ECGs and audiometry, at regular intervals.”
He added that microbiological checks are done at the end of the intensive phase and at treatment completion. For drug-resistant cases, cultures are monthly for six months, then every three months. If bacteria persist, treatment is adjusted immediately.
Each patient is tracked digitally through the Ni-kshay system, which keeps a record of their treatment progress. Missed doses or follow-up visits automatically trigger alerts, prompting community health workers to make home visits or calls.
This helps prevent treatment interruptions that could lead to relapse or drug resistance.
“Even after treatment, patients are advised to have checkups at six and twelve months,” he said. “Drug-resistant patients may need monitoring for one to two years.”
Through this structured process—diagnosis, treatment, monitoring, and post-treatment follow-up—he observed that the public system ensures patients are supported at every stage while minimising relapse and drug resistance.
The doctor emphasised that patient support and outreach are critical. “Financial assistance through the Nikshay Poshan Yojana, providing ₹1,000 per month, helps patients with nutrition and travel during treatment,” he said.
He also highlighted digital tools. SMS reminders, mobile apps, and video DOT are increasingly used to ensure adherence, especially for migrant populations or the urban poor who may struggle with regular clinic visits.
“Women, migrants, and slum dwellers often delay seeking care or have lower treatment completion rates,” he noted.
Nutrition support, counselling, and engagement of community TB champions reduce stigma and encourage adherence within these vulnerable groups, he added.
Private sector integration is also key. “A large share of TB care happens in the unregulated private sector. Strengthening linkages between private providers, public labs, and digital tools ensures that patients are not lost in the system and receive continuous care,” he observed.
Reflecting on the way forward, he noted, “The next major advances in TB control will come less from new drugs and more from better outreach, nutrition support, stigma-free awareness, and care models that fit the needs of women, migrants, and the urban poor.”
