Published Nov 14, 2025 | 7:00 AM ⚊ Updated Nov 14, 2025 | 7:00 AM

?")
AMR has serious consequences for individuals, healthcare systems, and economies. AMR leads to prolonged hospital admissions, increased healthcare costs, and higher costs in second-line treatments. (Shutterstock)
Synopsis: The latest Kerala Antimicrobial Resistance Surveillance Network annual report 2025 showed that while a few superbugs continue to challenge hospitals, subtle declines in resistance among key pathogens suggest that Kerala’s sustained surveillance and stewardship efforts may be paying off.
The latest Kerala Antimicrobial Resistance Surveillance Network (KARS-Net) annual report 2025, capturing data from 47 laboratories across 13 districts in 2024, paints a cautiously optimistic picture. While stubborn superbugs like Klebsiella and Staphylococcus aureus continue to challenge hospitals, subtle declines in resistance among key pathogens suggest that Kerala’s sustained surveillance and stewardship efforts may be paying off.
Compared to the previous year, resistance to critical drugs such as carbapenems and colistin has edged down in several bacterial species, and the state has significantly expanded its AMR monitoring network — a vital step toward early detection and containment.
It seems Kerala’s battle against antimicrobial resistance is showing glimmers of progress — but the war is far from over.
Alarm bells continue to ring over persistently high levels of ESBL-producing E. coli and Klebsiella strains, and the emergence of linezolid resistance among Enterococcus isolates points to new threats on the horizon.
The state’s latest antimicrobial resistance (AMR) surveillance data paints a mixed picture — while the state has significantly expanded its monitoring network, the patterns of bacterial resistance remain deeply concerning.
The 2025 report marks a significant expansion in Kerala’s AMR monitoring network, reflecting the growing strength of KARS-Net.
Covering data from 1 January to 31 December 2024, the report draws from 47 surveillance laboratories across 13 districts — an impressive rise from the 34 laboratories in 11 districts that contributed to the 2024 report.
KARSNET Report 2025
During this period, antimicrobial susceptibility (AST) data for 62,087 priority pathogens were collected, compared to 45,397 in the previous year, highlighting both a broader reach and enhanced diagnostic capacity.
After data deduplication, 55,640 unique patient isolates were analysed, a marked increase from 40,323 in 2023.
Of these, 45 percent (25,176) were from males and 55 percent (30,441) from females, with gender data unavailable for a small fraction of samples. Out of the 55,640 isolates, 45 percent were from in-patients (IPD), 45 percent from out-patients (OPD) and 10 percent from patients in Intensive care units (ICU)
Yet, the core findings reveal that some of the deadliest bacteria are holding their ground — and in some cases, showing no signs of retreat.
To understand what these findings mean, it helps to know what “isolated pathogens” are.
When patients develop infections, samples are collected and tested in laboratories. The bacteria that grow from these samples are called isolates, and identifying them helps doctors understand which organisms are causing infections and how resistant they are to antibiotics.
This surveillance is crucial for tracking AMR, a global health threat that renders common antibiotics ineffective.
According to the latest report, Escherichia coli (E. coli) remains the most common pathogen isolated from clinical samples, accounting for 40.4 percent of all bacteria detected in 2024 — almost identical to 40 percent in 2023.
E. coli was found to be the leading cause of urinary infections (58%), and it also topped the list of bacteria isolated from outpatients, inpatients, and intensive care units. This pattern mirrors the previous year’s data, underscoring how persistently this organism dominates infections in Kerala.
Klebsiella species, another high-priority pathogen, maintained a worrisome presence in bloodstream infections — accounting for 24 percent of isolates in 2024, compared to 26 percent in 2023.
The bacterium was also the most common organism found in other sterile body fluids.
Both E. coli and Klebsiella are known for their ability to develop resistance to multiple antibiotics, including carbapenems — a last-resort class of drugs used when other antibiotics fail.
The report revealed that nine percent of E. coli and 43 percent of Klebsiella isolates from blood were carbapenem-resistant (CRE) in 2024. While the Klebsiella figure has remained static since 2023, E. coli’s resistance has dropped slightly from 12 percent to nine percent.
Despite that minor improvement, the continued high rate of resistance in Klebsiella is alarming, as it suggests that hospital-acquired infections remain difficult to treat.
The situation with Staphylococcus aureus, a bacterium that commonly causes skin and wound infections, also demands attention. The proportion of methicillin-resistant S. aureus (MRSA) — a strain resistant to several key antibiotics — stood at 32 percent in 2024, nearly identical to 33 percent in 2023.
This shows that MRSA continues to be a persistent problem across hospital settings, especially for patients with surgical wounds or those using invasive devices.
Similarly, Enterococcus species — bacteria commonly found in the intestines that can cause severe infections in hospitalised patients — have maintained a stable three percent resistance rate to vancomycin, one of the strongest available antibiotics.
While the figure has not worsened since 2023, the presence of vancomycin-resistant strains is still a cause for vigilance, as treatment options for such infections are extremely limited.
On a positive note, the reports highlight improvements in the quality and consistency of AMR data collection.
More laboratories have adopted internal quality control systems and standardised testing protocols under the guidance of the National Centre for Disease Control (NCDC).
The number of centres performing advanced tests such as colistin broth microdilution (BMD) — used to assess resistance to colistin, a last-resort antibiotic — has also increased. Monthly feedback to network laboratories has helped improve the completeness and reliability of patient and testing data.
In summary, while Kerala’s AMR surveillance network has grown stronger and more comprehensive, the bacterial resistance trends reveal a persistent and serious challenge.
E. coli continues to dominate infections, and Klebsiella’s high level of carbapenem resistance remains a major threat to patient safety. Stable MRSA and vancomycin-resistant Enterococcus rates suggest the problem has plateaued rather than improved.
The state’s steady progress in expanding its surveillance network is commendable. Still, the data make one thing clear: Without stronger infection control, antibiotic stewardship, and rational prescription practices, Kerala risks seeing these pathogens become even harder to control in the years ahead.
Kerala has emerged as India’s frontrunner in tackling AMR — a mounting global public health crisis that threatens to render infections untreatable and jeopardise modern medicine.
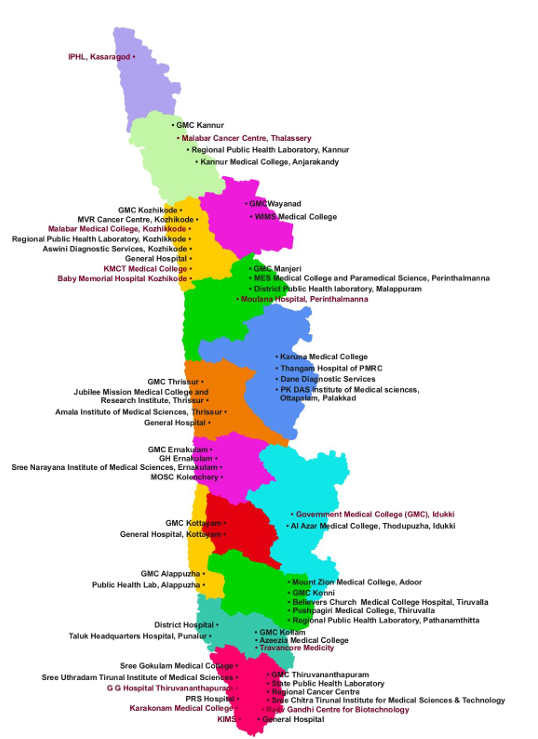
Institutions in the Kerala AMR Surveillance Network
Through its pioneering Kerala Antimicrobial Resistance Strategic Action Plan (KARSAP), launched in 2018, the state became the first in India to conceptualise and implement a comprehensive subnational AMR action plan.
AMR, often described as the “silent pandemic,” arises when bacteria, viruses, fungi, and parasites evolve to resist the drugs designed to kill them.
This leads to prolonged illness, higher treatment costs, and, in severe cases, fatalities. Kerala recognised early that only a “One Health” approach — integrating human, animal, and environmental health — can effectively counter this multifaceted threat.
To measure and monitor the magnitude of AMR in the state, Kerala established the Kerala Antimicrobial Resistance Surveillance Network (KARS-NET) in 2018, with the Department of Microbiology at Government Medical College, Thiruvananthapuram, as the state nodal centre.
Starting with just 10 laboratories, KARS-NET has grown into India’s largest state-level AMR surveillance network, now encompassing 59 laboratories across 14 districts, including 12 government medical colleges, 14 government hospitals, 20 private medical colleges, and several private and semi-autonomous laboratories.
With technical support from the World Health Organisation (WHO) and the National Centre for Disease Control (NCDC), KARS-NET integrates into the WHO’s Global Antimicrobial Resistance Surveillance System (GLASS), sharing data since 2021.
The state again made history in 2022 by becoming the first Indian state to release its own antibiogram— a comprehensive summary of antimicrobial susceptibility patterns across the state.
The KARS-NET antibiograms for 2021, 2022, and 2023 revealed that resistance trends among key bacterial pathogens varied significantly between healthcare centres, underlining the need for localised data-driven strategies.
Later, in a landmark development, the Ernakulam district released India’s first district-level antibiogram in 2024, adopting a hub-and-spoke model for AMR surveillance.
KARS-NET currently monitors nine key priority pathogens responsible for high antibiotic resistance rates and common infections:
1. Staphylococcus aureus
2. Enterococcus species
3. Klebsiella species
4. Escherichia coli
5. Acinetobacter species
6. Pseudomonas species
7. Salmonella enterica serovars Typhi and Paratyphi
8. Shigella species
9. Vibrio cholerae
Recognising India’s status as one of the world’s largest antibiotic consumers — with a usage rate of 13.3 defined daily doses per 1,000 people per day — the state has intensified its fight against misuse and resistance through KARSAP’s multi-pronged strategy.
The plan focuses on promoting judicious antibiotic use via hospital-based stewardship programs, strengthening infection control and hygiene practices, enhancing education and training for healthcare workers and the public, supporting research into new antimicrobials and rapid diagnostics, tightening regulatory oversight on antibiotic sales, and driving public awareness campaigns on antimicrobial resistance (AMR) and its prevention.
Kerala’s expanding AMR surveillance network and early signs of declining resistance mark encouraging progress in a long, uphill battle. But the stubborn resilience of pathogens like Klebsiella and MRSA is a reminder that the fight against antimicrobial resistance demands constant vigilance.
Only through sustained surveillance, rational antibiotic use, and stronger infection control can Kerala turn these small victories into lasting public health protection.
(Edited by Muhammed Fazil.)
