
Published Jan 16, 2026 | 7:00 AM ⚊ Updated Jan 24, 2026 | 5:57 PM

")
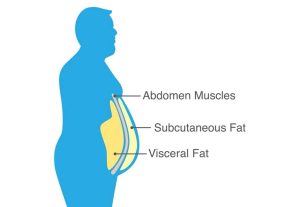
India's obesity epidemic. Representative image. (iStock)
Synopsis: States like Tamil Nadu, Goa, and Karnataka report the highest prevalence rates. Tamil Nadu, for instance, shows an age-standardised diabetes prevalence of 8,299.55 per 100,000 people.
Obesity (including visceral obesity) has rapidly increased within a generation in India, and is spreading to its villages and even children. This rise will result in catastrophic increases in healthcare spending at the individual and country-level.
![]()
The findings of India’s fifth National Family Health Survey (NFHS-5), conducted between 2019 and 2021, narrate a story of an impending public health crisis. While approximately one in four Indian adults is now classified as overweight or obese, these headline figures mask a more complex and alarming structural reality.
By analysing data from over 744,000 adults, the NFHS-5 reveals that India’s obesity epidemic differs fundamentally from Western models, primarily due to the specific ways the Indian population accumulates fat.
Historically, obesity has been measured via Body Mass Index (BMI). However, NFHS-5 introduced the measurement of waist circumference, a more accurate marker for visceral fat — the “hidden” fat stored around internal organs.
The results were startling: while BMI-based obesity affects 6.4% of women and 4% of men, abdominal obesity affects 39.6% of women and 11.9% of men.
This disparity highlights a crucial epidemiological pattern: Indian women preferentially accumulate visceral and upper-body fat even at lower overall body weights. A woman with a “normal” or slightly “overweight” BMI (E.g., 26 $kg/m^2$) may still carry metabolically hazardous abdominal fat. This explains why cardiovascular disease and type 2 diabetes often strike Indian populations with an intensity that standard BMI statistics fail to predict.
How does India’s obesity profile differ from that of the West? Several critical distinctions emerge.
First, the speed of epidemiological transition: Western nations experienced gradual increases in obesity prevalence over 60+ years (1950s-2010s); India experienced comparable increases in less than 30 years.
Second, the metabolic phenotype: Indian obesity concentrates in visceral and upper-body depots at lower overall BMI, creating more severe metabolic dysfunction per unit of body weight.
Third, the overlap with infectious disease and malnutrition: while Western obesity emerged in the context of universal adequate nutrition, Indian obesity coexists with pockets of continued malnutrition, complicating epidemiology.
Fourth, the healthcare infrastructure gap: Western nations developed healthcare systems to screen for and manage obesity progressively; India must rapidly build such infrastructure at scale with limited resources.
A final consideration: cultural and behavioural factors. The rapid adoption of Western dietary patterns, high in ultra-processed foods, refined carbohydrates, and vegetable oils, low in whole grains and plant fibre, occurred faster in India than health systems could adapt.
Simultaneously, urbanisation displaced traditional occupations requiring substantial physical activity, replacing them with sedentary desk work and motorised transportation. Traditional Indian dietary wisdom, built over millennia around seasonal produce, legumes, and modest portions, was displaced within a single generation.
The data reveals a significant “geographic lottery” regarding metabolic health. While the national average for overweight/obesity stands at 24%, state-level prevalence fluctuates wildly from 8% to 50%.
• Southern dominance: States like Tamil Nadu, Goa, and Karnataka report the highest prevalence rates. Tamil Nadu, for instance, shows an age-standardised diabetes prevalence of 8,299.55 per 100,000 people.
• Eastern/Northeastern resilience: These regions currently show lower prevalence, likely due to differences in dietary patterns, physical activity, and economic development stages.
Perhaps most alarming is the rapid narrowing of the rural-urban divide. Obesity was once considered a “rich man’s disease” or an urban luxury, but the gap is closing. In the short interval between NFHS-4 (2015-16) and NFHS-5 (2019-21), overweight/obesity rates in rural areas surged:
• Rural women: Rose from 8.6% to 19.7%
• Rural men: Rose from 7.3% to 19.3%
This acceleration is driven by the “nutrition transition”, the rapid penetration of ultra-processed foods, motorised transport, and sedentary labour into the heart of rural India.
The burden is not limited to adults. The prevalence of overweight children under five years old increased from 2.1% to 3.4% in just five years. This “doubling trajectory” suggests that the generation entering adulthood between 2040 and 2050 will face an unprecedented epidemic of chronic metabolic conditions.
The NFHS-5 data serve as a critical warning for policymakers. The transition of obesity from a localised urban issue to a nationwide structural crisis, defined by high metabolic risk at low BMI, requires a shift in healthcare strategy.
Focus must move beyond general weight loss to the management of visceral fat and the regulation of ultra-processed food environments, particularly in rural and pediatric populations.
(Edited by Majnu Babu).
